MPOX SAFETY INFORMATION (Sourced from CDC, DHS, EPA, CA Department of Health, LA County Department of Health, WHO)
Mpox Virus (MPXV) is a zoonotic virus (a virus that originates in animals) that belongs to the same group of viruses as the Variola major virus, which cause the human disease known as smallpox. MPXV causes a disease very similar to, but generally less severe, than smallpox. MPXV is native to Africa, and cases have been relatively rare in Europe and North America.
Historically, MPXV has not generally been associated with significant human-to human transmission. However, this has not been true of the current outbreak. Since the current outbreak began on or around May 13, 2022, MPXV cases have been reported in multiple countries, including the United States. The Center for Disease and Control Prevention (CDC) is currently working to identify why this mpox outbreak appears to be spreading differently than past outbreaks, possibly because it is more infectious or is transmitting in a novel way. The current MPXV outbreak has been declared both a global health emergency by the World Health Organization and a national health emergency by the Biden Administration.
General Transmission:
- Transmission occurs when a person comes into contact with the virus from an animal, human, or materials contaminated with the virus. The virus enters the body through broken skin, the respiratory tract, or other mucous membranes such as the rectum, eyes, genitals, and oral cavity.
- Person-to-person transmission occurs primarily through respiratory droplets, direct contact with body fluids or lesion material, and indirect contact with lesion material via contaminated fomites.
- Person-to-person transmission has been reported in previous outbreaks but was not common. Person-to-person transmission has been more common in the current outbreak than in the past. The mechanism for this is unknown.
- Mutations have been identified in the current outbreak strain that may enhance transmissibility relative to previous versions of the virus. The R0 of the current outbreak is not currently known. Past outbreaks have had an R0 of 0.96, which means the virus generally burned itself out without intervention or controls.
- People can be contagious before a visible rash appears and can continue shedding the virus weeks after symptoms have dissipated.
Environmental Transmission:
- While the current outbreak is primarily spreading through directed skin-to-skin contract, MPVX can also be spread through contaminated surfaces and materials. Surfaces and materials can become contaminated with lesion material, body fluids, or respiratory droplets.
- Because it is a large Orthopoxvirus, MPXV is quite stable in the environment. MPXV-contaminated surfaces and materials can remain contagious for months to years if not disinfected.
- For soft surfaces and materials, it is recommended that you either destroy them or wash them with a hospital grade detergent and chlorine. Please review the CDC’s guidance for mpox in healthcare environments for more information on laundering recommendations.
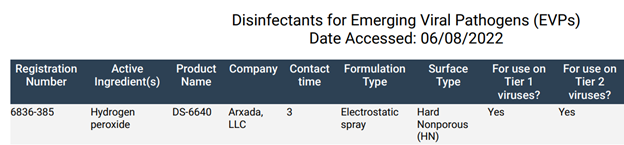
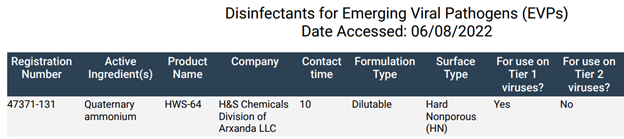
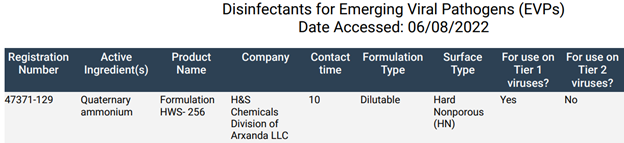
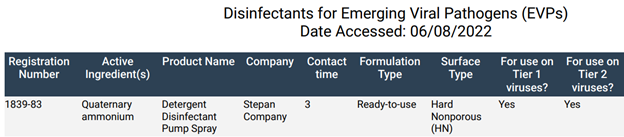
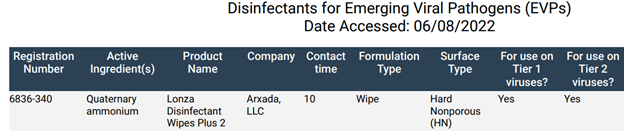
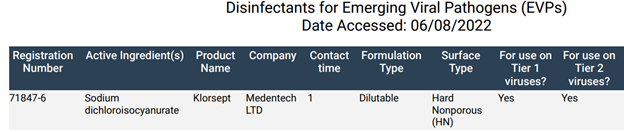
- For hard surfaces and materials, clean and disinfect using a disinfectant listed on EPA’s EVP List Q. The EPA has stated the following: “While there are no disinfectants registered for use against mpox, all products on the List of Disinfectants for Emerging Viral Pathogens (EVP) have been tested against viruses that are more difficult to kill than mpox.” The EPA’s EVP List Q was published in May of 2022 and lists the approved disinfectants and contact times.
- Servicon’s disinfectant products are on the EPA’s EVP List Q and have been compiled at the end of this document for your convenience.
Symptoms:
- The general incubation period (time from infection to symptoms) is 3−17 days, but the incubation period has been as long as 34 days in past outbreaks.
- The infection typically presents with a short prodromal phase with influenza-like illness before classical MPXV disease symptoms such as rash appear. The prodromal period generally lasts 1-4 days, with symptoms including some or all of the following: fever, fatigue, headache, backache, mild to severe pulmonary lesions, anorexia, dyspnea, conjunctivitis, nasal discharge, swollen lymph nodes, chills and/or sweats, sore throat, cough, and shortness of breath.
- Following the prodromal phase, mild to severe rash/lesions may appear, lasting 2-4 weeks. The rash is typically confined to the trunk but may appear on the palms and soles of feet. Lesions can develop on mucous membranes, in the mouth, on the tongue, and on the genitalia. In the current outbreak, lesions on the genitalia and perianal lesions have been more common due to the outsized role of sexual transmission.
- In the current outbreak, disease has not always been accompanied by classical symptoms and may present as a light rash with or without typical lesions and with or without perceptible fever. In combination with the genital and perianal presentation in many cases, this may lead to misdiagnosis via confusion with sexually transmitted infections such as syphilis, chancroid, and herpes.
- Lymphadenopathy (lymph nodes with abnormal size, number, or consistency) is a key distinguishing feature of mpox.
- While past outbreaks generally had between a 1-17% case fatality rate, the current outbreak is less severe and is associated with <1% mortality.
- The most common long-term effect of infection is scaring from the lesions.
Case Definitions:
- A suspected case is defined as someone who presents with a new characteristic rash or lesions OR someone with a high clinical suspicion due to one of the following:
- (a) contact with a person or people with a similar appearing rash or who received a diagnosis of confirmed or probable mpox.
- (b) close or intimate in-person contact with individuals in a social network experiencing mpox activity, including men who have sex with men (MSM) who meet partners through an online website, digital application (“app”), or social event (e.g., a bar or party).
- (c) traveled outside the US to a country with high levels of mpox.
- (d) had contact with a dead or live wild animal or exotic pet that is an African endemic species or used a product derived from one (i.e., game meat, powders, creams, lotions).
- A confirmed case is defined as someone who has tested positive for mpox OR who’s clinical specimen has mpox present.
Prevention:
- Isolate a suspected or confirmed infected person from others. Extra precautions should be taken against direct contact with lesions until the lesions have crusted.
- Avoid contact with any surfaces or materials that have been in contact with a suspected or confirmed infected person.
- Practice good hand hygiene after contact with a suspected or confirmed infected person, such as washing your hands with soap and water or using an alcohol-based hand sanitizer.
- Perform decontamination (or destruction) of any surfaces or materials that have been in contact with a suspected or confirmed infected person.
- Decontamination procedures in non-healthcare environments are substantially the same as COVID-19 cleaning and disinfection protocols.
- Decontamination procedures in healthcare environments vary from COVID-19 cleaning and disinfection protocols, with added notes to avoid sweeping, dry dusting, and vacuuming prior to disinfection.
- Materials are not to be shaken, as it may cause virus partials on the materials to become airborne.
- Use personal protective equipment (PPE) when dealing with a suspected or confirmed infected person or when performing decontamination. The basic level of PPE controls are gloves, gowns, surgical masks, and eye protection.
- Healthcare environments with confirmed individuals should use respirators instead of surgical masks.
Vaccination & Treatments:
- Vaccination with smallpox vaccine (vaccinia virus) is reported to provide protection against 85% of MPXV infections.
- Two vaccines are licensed by the FDA for use in the United States. JYNNEOS (Bavarian Nordic A/S) is a two-dose nonreplicating MVA vaccine that is appropriate for use in individuals for whom the live vaccine is contraindicated. This vaccine is specifically licensed for MPXV by the FDA in addition to licensure for smallpox. ACAM2000 (Emergent) is a live vaccinia virus vaccine that can be used for MPXV, although it has not been specifically licensed for this use.
- The United States does not have a large supply of these vaccines. Vaccination guidelines are changing and depend on state and local rules. General guidance is to provide vaccinations to at-risk groups based on occupational exposure (first responders) or sexually active men who have sex with men (MSM).
- While there are no approved antivirals specific to MPXV, there are some therapeutic options that have been approved for use against smallpox that may be effective against MPXV, including post-exposure vaccination.
Servicon’s Disinfectant Products & Mpox Contact Time:
Maintex Peroxide RTU – 6836-385
Maintex Citra-Cide – 47371-131
Maintex Retaliate – 47371-129
Maintex Turnbo Kill RTE – 1839-83
SONO Disinfecting Wipes – 6836-340
PurTabs (Infection Prevention Electrostatic Sprayers) – 71847-6
Sources: Centers for Disease and Control, Department of Homeland Security, County of Los Angeles Public Health, California Department of Public Health, Environmental Protection Agency, World Health Organization.